


Ahead of this year’s virtual edition of the 4th World Bronchiectasis & Non-Tuberculous Mycobacteria (NTM) Conference, to be held on 16–19 December 2020, Porterhouse Medical would like to highlight the increasing incidence of bronchiectasis, its economic burden and the urgent need for improved disease management.
Disease characteristics and symptoms
Bronchiectasis is a chronic respiratory disease characterised by abnormal and often permanent dilatation of the bronchi (the main passageways that carry air to the lungs) [1].
Bronchial dilatation leads to impairment of mucociliary clearance (the respiratory system’s self-clearing mechanism), resulting in persistent infection, inflammation and further damage to the airways [2]. The interplay between acute disease exacerbations, chronic infection, inflammation and impaired mucociliary clearance drives a vicious cycle that results in injury to the bronchi and other structures within the lungs (Figure 1) [2, 3]. In severe cases, progressive airway damage can lead to impaired lung function that may progress to respiratory failure and death [4].
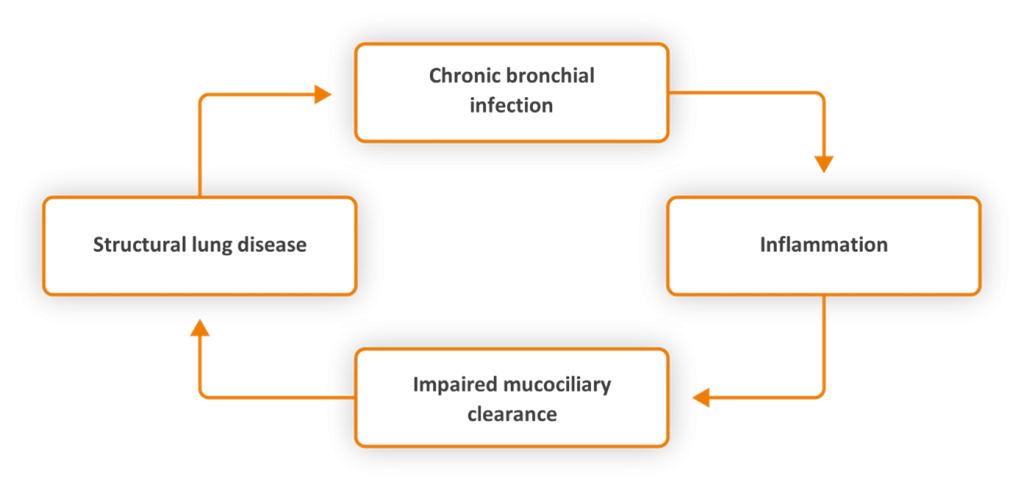
Figure 1. The ‘vicious cycle’ concept of bronchiectasis [2, 3]
A marked increase in disease prevalence and severity is observed in the elderly; however, mortality rates across all age groups are reported to be substantially higher in those with a diagnosis of bronchiectasis compared with the general population [5].
Patients with bronchiectasis usually present with cough, sputum production and recurrent chest infections, alongside other symptoms such as malaise, chest discomfort, haemoptysis (coughing of blood) and weight loss [6]. As the clinical presentation of bronchiectasis overlaps with other more common respiratory diseases, it is likely to be underdiagnosed, which makes it a challenge to determine the exact prevalence of the disease [7].
Non–cystic fibrosis bronchiectasis
Bronchiectasis is classified according to its association with cystic fibrosis (CF). In patients in whom CF has been excluded, the disease is referred to as non-CF bronchiectasis (NCFB) [8].
During the pre-antibiotic era, severe infections such as pneumonia and tuberculosis were the predominant causes of NCFB, particularly in the least developed countries [1, 8]. The introduction of antibiotics was expected to reduce the clinical burden of NCFB over time by suppressing bacterial load in these patients; however, the emergence of resistant bacteria has limited their efficacy [9].
Unlike other inflammatory airway diseases, such as asthma and chronic obstructive pulmonary disease (COPD), NCFB has historically received limited research attention [10] and therefore is described as a neglected disease [11]. As such, there are no licensed therapies for the treatment of NCFB; current treatment options focus only on improving airway clearance and reducing the impact of structural lung disease [1, 12].
The economic burden of NCFB is substantial, with annual costs in the USA approximating US$ 630 million [13]. Major drivers behind these costs are hospitalisations, the need for intensive care and the use of inhaled antibiotics [13–17]. Furthermore, because of the use of retrospective studies and the exclusion of outpatient expenses, management costs of NCFB are likely to be underestimated [18].
A brighter future
In the UK, a population-based study identified a year-on-year increase in the incidence and prevalence of NCFB from 2004 to 2013. These findings were observed in almost all age groups, with the most rapid increase seen in women over 70 years of age [5].
The increasing incidence of NCFB has driven a surge of interest in the disease, leading to new studies into the causal mechanisms of the disease and the generation of international treatment guidelines [12, 19].
In 2017, the European Respiratory Society (ERS) published the first evidence-based recommendations for the management of adult bronchiectasis. These recommendations aim to improve the quality of patient care and promote safe, effective and cost-effective treatment [12].
Novel pathogenic pathways, particularly those relating to inflammation and ciliary dysfunction, have also been discovered and could lead to new therapeutic opportunities in the future [1]. Furthermore, four clinical phenotypes in bronchiectasis have been identified following secondary analysis of outpatient data across five European databases [20]. Significantly, patients with these clinical phenotypes have distinctly different patterns of sputum biomarkers, quality of life scores and long-term clinical outcomes. The establishment of these clinical phenotypes represents a step towards individualised patient management and could also help to selectively include patients in clinical trials who are more likely to respond to treatment [1, 20].
Despite this renewed research attention and investment, we are still a long way from fully understanding NCFB. Unravelling the heterogeneity of the disease remains a key research priority and will be paramount to the development of novel therapeutic strategies that may improve disease management and patient outcomes in the future. As the incidence and prevalence of NCFB continue to increase with an ageing population, this must be reflected in the provision of care for patients with this disease [3, 5].
The impact of COVID-19 on patients with bronchiectasis
As bronchiectasis is a chronic respiratory condition, patients with the disease are classified as clinically vulnerable (or clinically extremely vulnerable if they have severe disease). This means that, compared with the general population, they are at higher risk of becoming seriously ill if they contract COVID-19 [21]. For additional information, please see the Government’s guidance on shielding and protecting clinically extremely vulnerable individuals from COVID-19 [22].
Additionally, the COVID-19 pandemic has further limited the treatment options available to patients with bronchiectasis. Routine appointments (such as annual treatment reviews) have been postponed for some individuals, and pulmonary rehabilitation courses have been temporarily paused [23]. As efforts to develop a COVID-19 vaccine continue, it is hoped that routine care for patients with bronchiectasis can soon return to normal.
References
- Chalmers JD, Chang AB, Chotirmall SH et al. Bronchiectasis. Nat Rev Dis Primers 2018; 4 (1): 45.
- Cole PJ. Inflammation: A two-edged sword — the model of bronchiectasis. Eur J Respir Dis Suppl 1986; 147: 6–15.
- Chandrasekaran R, Aogáin MM, Chalmers JD et al. Geographic variation in the aetiology, epidemiology and microbiology of bronchiectasis. BMC Pulm Med 2018; 18 (1): 83.
- Chalmers JD, Geominne P, Aliberti S et al. The bronchiectasis severity index. An international derivation and validation study. Am J Respir Crit Care Med 2014; 189 (5): 576–585.
- Quint JK, Millett ERC, Joshi M et al. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: A population-based cohort study. Eur Respir J 2016; 47 (1): 186–193.
- Chalmers JD, Aliberti S and Blasi F. Management of bronchiectasis in adults. Eur Respir J 2015; 45 (5): 1446–1462.
- Tsang KW. Solutions for difficult diagnostic cases of acute exacerbations of chronic bronchitis. Chemotherapy 2001; 47 (Suppl 4): 28–38; discussion 53–54.
- Goeminne P and Dupont L. Non-cystic fibrosis bronchiectasis: Diagnosis and management in 21st century. Postgrad Med J 2010; 86 (1018): 493–
- Donovan T, Felix LM, Chalmers JD et al. Continuous versus intermittent antibiotics for bronchiectasis. Cochrane Database Syst Rev 2018; 6 (6): CD012733.
- Tsang KW and Bilton D. Clinical challenges in managing bronchiectasis. Respirology 2009; 14 (5): 637–650.
- Goeminne PC and De Soyza A. Bronchiectasis: How to be an orphan with many parents? Eur Respir J 2016; 47 (1): 10–13.
- Polverino E, Geominne PC, McDonnell MJ et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J 2017; 50 (3): 1700629.
- Weycker D, Edelsberg J, Oster G et al. Prevalence and economic burden of bronchiectasis. Clin Pulm Med 2005; 12 (4): 205–209.
- Ringshausen FC, de Roux A, Pletz MW et al. Bronchiectasis-associated hospitalizations in Germany, 2005–2011: A population-based study of disease burden and trends. PLoS One 2013; 8 (8): e71109.
- Seitz AE, Olivier KN, Steiner CA et al. Trends and burden of bronchiectasis-associated hospitalizations in the United States, 1993–2006. Chest 2010; 138 (4): 944–949.
- de la Rosa D, Martínez-Garcia MA, Olveira C et al. Annual direct medical costs of bronchiectasis treatment: Impact of severity, exacerbations, chronic bronchial colonization and chronic obstructive pulmonary disease coexistence. Chron Respir Dis 2016; 13 (4): 361–371.
- Gursel G. Does coexistence with bronchiectasis influence intensive care unit outcome in patients with chronic obstructive pulmonary disease? Heart Lung 2006; 35 (1): 58–65.
- Goeminne PC, Hernandez F, Diel R et al. The economic burden of bronchiectasis – known and unknown: A systematic review. BMC Pulm Med 2019; 19 (1): 54.
- Chalmers JD and Chotirmall SH. Bronchiectasis: New therapies and new perspectives. Lancet Respir Med 2018; 6 (9): 715–726.
- Aliberti S, Lonni S, Dore S et al. Clinical phenotypes in adult patients with bronchiectasis. Eur Respir J 2016; 47 (4): 1113–1122.
- National Health Service. Who’s at higher risk from coronavirus. Available at: https://www.nhs.uk/conditions/coronavirus-covid-19/people-at-higher-risk/whos-at-higher-risk-from-coronavirus/. Accessed November 2020.
- UK. Guidance on shielding and protecting people who are clinically extremely vulnerable from COVID-19. Available at: https://www.gov.uk/government/publications/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19. Accessed November 2020.
- British Lung Foundation. Coronavirus and living with a lung condition. Available at: https://www.blf.org.uk/support-for-you/coronavirus/people-living-with-lung-condition. Accessed November 2020.
 Author: Laura Hemmings
Author: Laura Hemmings
Associate Medical Writer | Porterhouse Medical